|
|
Prostate-Specific Antigen (PSA) Test Information
Fill out our online form for a P.S.A. testing
inquiry: Prostate-Specific Antigen (PSA) Test
Form
- What is the Prostate-Specific
Antigen (PSA) Test?
PSA is a protein produced by the cells of the
prostate gland. The prostate-specific antigen (PSA) test measures the level
of PSA in the blood. A blood sample is drawn and the amount of PSA is
measured in a laboratory. When the prostate gland enlarges, PSA levels in
the blood tend to rise. PSA levels can rise due to cancer or benign (not
cancerous) conditions. Because PSA is produced by the body and can be used
to detect disease, it is sometimes called a biological marker or tumor
marker.
As men age, both benign prostate conditions and
prostate cancer become more frequent. The most common benign prostate
conditions are prostatitis (inflammation of the prostate) and benign
prostatic hyperplasia (BPH) (enlargement of the prostate). There is no
evidence that prostatitis or BPH cause cancer, but it is possible for a man
to have one or both of these conditions and to develop prostate cancer as
well.
Although Elevated PSA Advanced Test levels alone do not give doctors enough
information to distinguish between benign prostate conditions and cancer,
the doctor will take the result of this test into account in deciding
whether to check further for signs of prostate cancer.
Back to Top
- Why is the PSA test performed?
As with many other routine
blood tests, PSA is measured from a small sample of blood. Once a blood
sample is taken, the level of PSA in the sample is measured by an accurate
laboratory method called an
immunoassay. The
results are usually reported in ng/ml, shorthand for
nanograms per milliliter.
The U.S. Food and Drug Administration (FDA) has
approved the PSA test for use in conjunction with a digital rectal exam (DRE)
to help detect prostate cancer in men age 50 and older. During a DRE, a
doctor inserts a gloved finger into the rectum and feels the prostate gland
through the rectal wall to check for bumps or abnormal areas. Doctors often
use the PSA test and DRE as prostate cancer screening tests in men who have
no symptoms of the disease.
The FDA has also approved the PSA test to monitor
patients with a history of prostate cancer to see if the cancer has come
back (recurred). An elevated PSA level in a patient with a history of
prostate cancer does not always mean the cancer has come back. A man should
discuss an elevated Elevated PSA Advanced Test level with his doctor. The doctor may recommend
repeating the PSA test or performing other tests to check for evidence of
recurrence.
It is important to note that a man who is receiving
hormone therapy for prostate cancer may have a low PSA reading during, or
immediately after, treatment. The low level may not be a true measure of PSA
activity in the patient’s body. Patients receiving hormone therapy should
talk with their doctor, who may advise them to wait a few months after
hormone treatment before having a PSA test.
Back to Top
-
For whom might a PSA screening test be recommended? How
often is testing done?
The benefits of screening for prostate cancer are
still being studied. The National Cancer Institute (NCI) is currently
conducting the Prostate, Lung, Colorectal, and Ovarian Cancer Screening
Trial, or PLCO trial, to determine if certain screening tests reduce the
number of deaths from these cancers. The DRE and PSA are being studied to
determine whether yearly screening to detect prostate cancer will decrease
one’s chance of dying from prostate cancer.
Doctors’ recommendations for screening vary. Some
encourage yearly screening for men over age 50; others recommend against
routine screening; still others counsel men about the risks and benefits on
an individual basis and encourage patients to make personal decisions about
screening.
Several risk factors increase a man’s chances of
developing prostate cancer. These factors may be taken into consideration
when a doctor recommends screening. Age is the most common risk factor, with
more than 96 percent of prostate cancer cases occurring in men age 55 and
older. Other risk factors for prostate cancer include family history and
race. Men who have a father or brother with prostate cancer have a greater
chance of developing prostate cancer. African American men have the highest
rate of prostate cancer, while Native American men have the lowest.
Back to Top
- How are PSA results reported?
PSA test results report the level of
PSA detected in the blood. There are several different ways to measure PSA.
Most physicians think that the "normal range" is between 0 and 4.0 nanograms
per milliliter (ng/ml) for the most common PSA tests. (Because some PSA
tests have different normal ranges, you should check with your physician on
this point.) A PSA level of 4 to 10 ng/ml
is considered slightly elevated; levels between 10 and 20 ng/ml are
considered moderately elevated; and anything above that is considered highly
elevated. The lab's "normal" upper level is simply a cutoff point used to
separate men who are less likely to have prostate cancer from those for whom
further prostate cancer testing may be appropriate, depending upon the
circumstances. The higher a man’s PSA level, the more likely it is
that cancer is present. But because various factors can cause PSA levels to
fluctuate, one abnormal PSA test does not necessarily
indicate a need for other diagnostic tests. When PSA levels continue to rise
over time, other tests may be indicated.
Back to Top
- What causes PSA to rise?
The level of PSA in the
bloodstream may be elevated by an process that leads to an increase in the
number of cells making PSA or to a breakdown of the normal barriers in the
prostate that prevent much PSA from getting into the bloodstream. The most
common condition leading to a high PSA is benign (noncancerous) enlargement
of the prostate, called benign prostatic hyperplasia
(BPH). BPH is very common in men over the age of 50 and may lead to
difficulty with urination. Infection or inflammation in the prostate, called
prostatitis, may also cause elevation
of PSA by damaging the PSA barrier in the prostate. In
addition, some diagnostic tests, such as a needle
biopsy of the prostate, may increase
PSA levels for several weeks. It does not appear that a routine
digital rectal examination
(DRE) of the prostate by the doctor's finger causes an elevation of the PSA.
Both BPH and prostate cancer
are common in men over the age of 50. In addition, there is a lot of overlap
in blood PSA levels between men with BPH and those with early prostate
cancer. These factors limit the usefulness of PSA as a tool for detecting
curable prostate cancer. Many patients who have a PSA level higher than 4 ng/ml
will eventually be found not to have prostate cancer. These men have a
"false-positive" test. If PSA is tested on men with BPH but no prostate
cancer, as many as one-third to one-half of such men will have an elevated
PSA. Their PSA results, however, are generally in the 4 to 10 ng/ml range.
Back to Top
- What if the test results show an elevated PSA level?
A man should discuss elevated PSA test results with
his doctor. There are many possible reasons for an elevated PSA level,
including prostate cancer, benign prostate enlargement, inflammation,
infection, age, and race. If there are no other indicators that suggest
cancer, the doctor may recommend repeating DRE and PSA tests regularly to
monitor any changes.
If a man’s PSA levels have been increasing or if a
suspicious lump is detected in the DRE, the doctor may recommend other
diagnostic tests to determine if there is cancer or another problem in the
prostate. A urine test may be used to detect a urinary tract infection or
blood in the urine. The doctor may recommend imaging tests, such as
ultrasound (a test in which high-frequency sound waves are used to obtain
images of the kidneys and bladder), x-rays, or cystoscopy (a procedure in
which a doctor looks into the urethra and bladder through a thin, lighted
tube). Medicine or surgery may be recommended if the problem is BPH or an
infection.
If cancer is suspected, the only way to tell for sure
is to perform a biopsy. For a biopsy, samples of prostate tissue are removed
and viewed under a microscope to determine if cancer cells are present. The
doctor may use ultrasound to view the prostate during the biopsy, but
ultrasound cannot be used alone to tell if cancer is present.
Back to Top
- What are some of the limitations of the PSA test?
- Detection does not always mean saving lives:
Even though the PSA test can detect small tumors, finding a small tumor
does not necessarily reduce a man’s chance of dying from prostate
cancer. PSA testing may identify very slow-growing tumors that are
unlikely to threaten a man’s life. Also, PSA testing may not help a man
with a fast-growing or aggressive cancer that has already spread to
other parts of his body before being detected.
- False positive tests: False positive test
results (also called false positives) occur when the PSA level is
elevated, but no cancer is actually present. False positives may lead to
additional medical procedures, with significant financial costs and
anxiety for the patient and his family. Most men with an elevated PSA
test turn out not to have cancer.
False positives occur primarily in men age 50 or
older. In this age group, 15 of every 100 men will have elevated PSA
levels (higher than 4 ng/ml). Of these 15 men, 12 will be false
positives and only three will turn out to have cancer.
- False negative tests: False negative test
results (also called false negatives) occur when the PSA level is in the
normal range even though prostate cancer is actually present. Most
prostate cancers are slow-growing and may exist for decades before they
are large enough to cause symptoms. Subsequent PSA tests may indicate a
problem before the disease progresses significantly.
In addition to false-positive tests, the PSA may be falsely negative -- that is, normal
even when prostate cancer is present. Some 30 to 40 percent of patients with
early-stage prostate cancer have a normal PSA. Repeating PSA tests once
every year may be useful to find some of the cancers in men who have a
normal PSA at first.
False-negative and false-positive
findings limit the value of PSA testing. Despite this, PSA testing has led
to an increase in the detection of prostate cancer.
Back to Top
- Why is the PSA test controversial?
Using the PSA test to screen men for prostate cancer
is controversial because it is not yet known if the process actually saves
lives. Moreover, it is not clear if the benefits of PSA screening outweigh
the risks of follow-up diagnostic tests and cancer treatments.
The procedures used to diagnose prostate cancer may
cause significant side effects, including bleeding and infection. Prostate
cancer treatment often causes incontinence and impotence. For these reasons,
it is important that the benefits and risks of diagnostic procedures and
treatment be taken into account when considering whether to undertake
prostate cancer screening.
Back to Top
- What research is being done to improve the PSA test?
Scientists are researching ways to distinguish
between cancerous and benign conditions, and between slow-growing cancers
and fast-growing, potentially lethal cancers. Some of the methods being
studied are:
- PSA velocity: PSA velocity is based on
changes in PSA levels over time. A sharp rise in the PSA level raises
the suspicion of cancer.
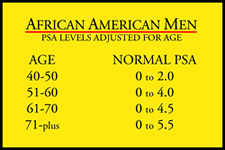
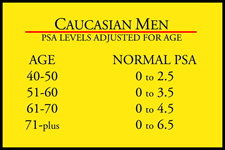
- Age-adjusted PSA: Age is an important
factor in increasing PSA levels. For this reason, some doctors use
age-adjusted PSA levels to determine when diagnostic tests are needed.
When age-adjusted PSA levels are used, a different PSA level is defined
as normal for each 10-year age group. Doctors who use this method
suggest that men younger than age 50 should have a PSA level below 2.5
ng/ml, while a PSA level up to 6.5 ng/ml would be considered normal for
men in their 70s. Doctors do not agree about the accuracy and usefulness
of age-adjusted PSA levels.
- PSA density: PSA density considers the
relationship of the PSA level to the size and weight of the prostate. In
other words, an elevated PSA might not arouse suspicion in a man with a
very enlarged prostate. The use of PSA density to interpret PSA results
is controversial because cancer might be overlooked in a man with an
enlarged prostate.
- Free versus attached PSA:
PSA circulates in the blood in two forms:
free or attached to a protein molecule. With benign prostate conditions,
there is more free PSA, while cancer produces more of the attached form.
Researchers are exploring different ways to measure PSA and to compare
these measurements to determine if cancer is present. In clinical practice, free PSA
serves as an additional tool to help decide which men need more
aggressive evaluation to check for prostate cancer, including a prostate
biopsy, and which men might be safely managed with observation including
serial exams and PSA tests over time. In men presenting with a high
standard total PSA test (certainly any value over 10) or with a
suspicious digital rectal examination of the prostate, there is no
recognized utility for obtaining an additional free PSA test. In most
such cases, prostate biopsy is indicated to rule out cancer. Free PSA
has been proposed as a secondary test in men with a slight elevation or
abnormality of the standard total PSA level, who otherwise have no
suspicion of prostate cancer on their physical exam, and who perhaps
have an enlarged prostate (BPH) which might also cause a mild elevation
of the PSA levels above normal. If the percent free PSA compared to
total PSA is high in such an individual, several preliminary clinical
studies have suggested that it might be safe to avoid a biopsy of the
prostate. This might be particularly beneficial in patients in whom
prostate biopsy is technically difficult, such as those who are on
medical anticoagulation (blood thinners) for a variety of cardiovascular
problems, or the man whose rectum has been surgically removed because of
rectal cancer. It should be emphasized throughout this discussion that
the proper use of free PSA is still a matter of scientific study and
debate. Any man with an abnormally elevated standard PSA test but a
"normal" percent free PSA who chooses, after careful consideration with
his or her physician, to avoid a prostate biopsy, should have careful
medical observation, including repeat PSA tests and prostate exams done
on a regular basis.
- Other screening tests: Scientists are
also developing screening tests for other biological markers, which are
not yet commercially available. These markers may be present in higher
levels in the blood of men with prostate cancer.
Back to Top
|

